
Key Takeaways:
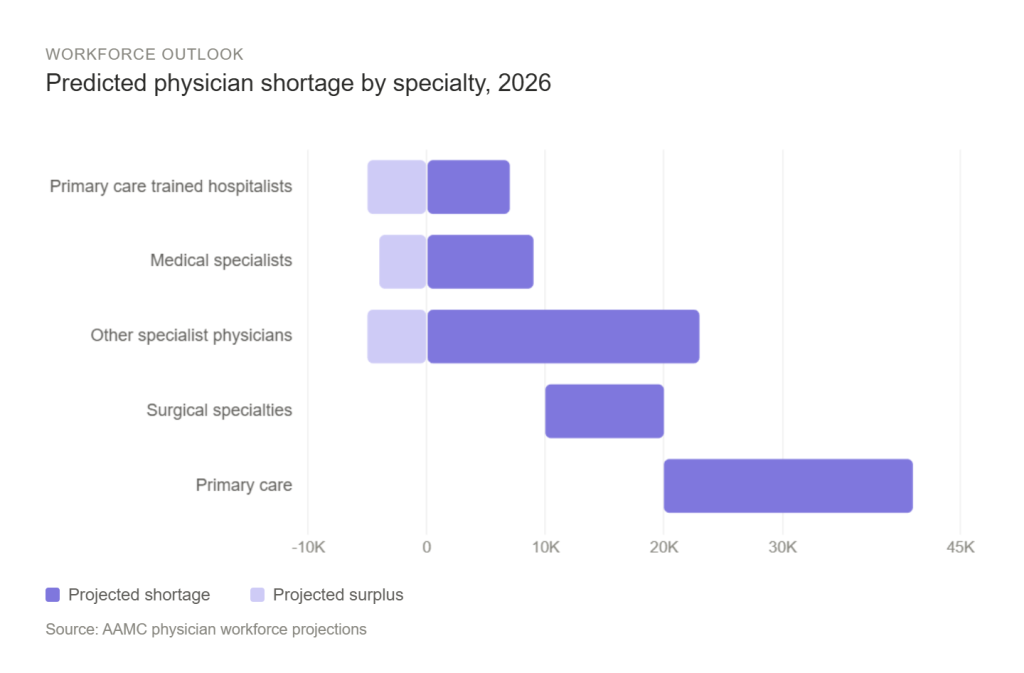
The U.S. faces a projected shortage of 86,000 physicians by 2036, with primary care experiencing deficits of up to 40,400 physicians, and surgical specialties facing shortages of up to 19,900 surgeons.
These shortages are driven by an aging population, rising chronic disease burden, and an undersupply of domestic medical school graduates relative to demand.
Rural and underserved communities have struggled to attract and retain physicians, making them disproportionately reliant on foreign-trained physicians – recent changes to immigration policy may further strain physician supply in the US.
Physician shortages may additionally drive locum tenens costs given projected limited physician demand, as well as increase uncompensated care and force service line reductions.
The Resident Physician Shortage Reduction Act (H.R. 3890) may help reduce reliance on foreign-trained physicians; however meaningful workforce relief will likely not materialize until the early 2030s.
Pathstone Partners specializes in helping healthcare organizations implement operational efficiencies that preserve care quality while controlling costs during workforce constraints.
The physician shortage confronting the United States threatens both the financial viability of healthcare organizations and the health of millions of Americans. According to the Association of American Medical Colleges, the US will face a shortage of between 13,500 and 86,000 physicians by 2036, with demand continuing to outpace supply under all scenarios. The shortage will also impact specialties disproportionately distribution, with primary care experiencing the most severe deficit, between 20,200 and 40,400 physicians by 2036, representing over 10% of the current 234,300 active primary care physicians nationwide. Surgical specialties will also face shortages of 10,100 to 19,900 surgeons, while psychiatry and mental health services are forecasted to see continued critical deficits as demand surges with a growing mental health crisis.
The Physician Bottleneck and an Aging Population
Multiple factors have created this physician labor crisis – the US population will grow by 8.4% through 2036, however the 65-and-older population will increase disproportionately by 34%, and those 75 and older increasing nearly 55%. Since older Americans utilize physician services at three to four times the rate of younger populations, demand growth also increases accordingly.
Meanwhile, the physician workforce itself is aging. Over 40% of currently active physicians will reach traditional retirement age within the next decade, threatening to remove more than a third of practicing physicians from the system. This retirement wave arrives precisely as demand for physicians accelerates, creating a compounding effect on healthcare systems and patients in need of care.
The pipeline for new physicians, however, remains constrained. Since 1997, CMS has maintained a cap on federally funded residency positions. While the Consolidated Appropriations Act of 2021 added 1,000 new positions, this falls far short of projected demand needed to account for both an aging physician workforce, and an aging general population. Even if medical school enrollment were expanded today, the 7- to 10- year training timeline means meaningful relief remains approximately a decade away. Geographic maldistribution further compounds this problem as physicians disproportionately concentrate in urban and suburban market, which leaves rural and low-income communities underserved regardless of national supply figures.
Both California and Congress have begun responding to a need to expand the physician pipeline, though the scale of the proposed solutions are still likely to remain short of the projected need. At the state level, California’s CalMedForce grant program has supported over 1,183 residency positions across 162 programs. Approximately 75% of residents trained in the state remain in California, making in-state training one of the most reliable tools for building a durable local workforce. At the federal level, bipartisan legislation has emerged to finally address the Medicare residency cap that has constrained supply since 1997.
The Resident Physician Shortage Reduction Act (H.R. 3890) would add 14,000 Medicare-funded residency positions over seven years, with 2,000 new slots annually from 2026 through 2032. The bill would also authorize $63.5 million in grant funding for rural hospitals seeking to launch new residency programs. However, if passed, the long training timeline means meaningful workforce relief would not materialize until the early 2030s at the earliest.
Immigration Policy and the Potential Impact on Vulnerable Communities
Recent immigration policy changes have also threatened to worsen the shortage where it hurts most. Analysis published in JAMA reveals that in fiscal year 2024, approximately 11,000 physicians, or nearly 1% of the national workforce, were sponsored for H-1B visas. Foreign-trained physicians fill critical gaps particularly in underserved communities – in US counties with the highest poverty levels, H-1B-sponsored physicians comprise 2% of the physician workforce, which is nearly four times higher than in low-poverty counties, and are also substantially more likely to enter specialties less attractive to US-trained physicians such as primary care and psychiatry.
Recent policy changes, including significant increases to visa-related fees, and in some states, administrative freezes on new applications, have raised some concerns for the future of hospitals which rely significantly on international physician recruitment – particularly those that are smaller or rural institutions that are already operating on thin margins.
Financial and Clinical Consequences
Physician shortages translate directly to financial pressure and compromised care. For example, research consistently shows that physician shortages correlate with worse chronic disease outcomes, lower cancer screening rates, and higher mortality. Additionally, capacity challenges also highlight the need to free cash to fund growth and meet patient demand.
Some examples of more immediate downstream effects for hospitals include:
- Uncompensated care rising as communities lose primary care access, forcing patients to delay treatment until conditions require expensive emergency department visits or hospitalizations.
- Service line reductions becoming inevitable when organizations cannot recruit or retain physicians in critical specialties.
- Rural hospitals may face choosing between maintaining money-losing service lines with expensive contract labor or discontinuing services entirely.
- Long-term increases in permanent physician compensation and locums tenens rates as organizations compete for limited talent.
- Patient outcomes decreasing due to longer wait times, delayed diagnoses, and reduced access to preventive care.
Strategic Solutions to Maximize Value
As physician shortages continue to strain healthcare organizations, Pathstone Partners has worked with clients to implement strategic operational improvements that maximize value from existing resources.
Our engagements have included reviewing and optimizing virtual care models that allow specialists to serve multiple locations efficiently and enable primary care physicians to consult remotely, therefore gaining more capacity from an existing physician base. A key insight from this work is that telehealth implementation is not one-size-fits-all. Organizations can choose from a spectrum of staffing models depending on their goals, resources, and patient population. Helping clients evaluate and plan across these phases is an important part of building a durable virtual care strategy.
By appropriately diverting lower-acuity cases, physicians are freed to focus on higher-acuity patients where their expertise is most needed, which improves resource utilization, the quality of care patients are able to receive, and provides meaningful operational improvement particularly for organizations already grappling with physician recruitment challenges.
Beyond workforce strategy, Pathstone also works across a wide variety of operational initiatives designed to free up cash flow, fund critical priorities, and help organizations meet growing patient demand, including supply chain restructuring, cost reduction, or revenue cycle improvements to help health systems unlock capital that can then be redeployed.
While the physician shortage represents a significant challenge, forward-thinking organizations can differentiate themselves through operational excellence. Those implementing strategic measures now will be better positioned to maintain care quality and ensure long-term financial sustainability.
Reach out to Pathstone Partners today to request a no-cost opportunity assessment and discover how we can help your organization plan for the future.